DAYTRANA (methylphenidate). ADHD PATCH
Watch Video at
Linton 54, 55
Pharm Chapter 20 Quizlet
NCLEX QUESTIONS Integumentary Disorders
Below is a link to NCLEX style Integumentary questions from the same site as the questions found on Aileen’s last test (Geriatrics)
Grade Worksheet HLPAE LVN Program
IV CALCULATIONS
IV CALCULATIONS
A physician’s order for IV therapy must include
- Type of Solution
- Quantity of Solution
- Time period for administration
- In some institutions,for Pediatric order, also includes mL/hr
Examples:
- Administer 1000mL of D5W at 125 mL/h
- Administer 1000mL 0.9% NS every 12 hours x 2 days
- Administer 500mL of D10W at 83 mL/h
- Administer 100mL of RL over 4 hours at 25 mL/h
Calculating gtts/ min for Gravity Flow IV Infusion
You need 3 pieces of information
- Total volume to be infused in mL
- Drop factor of tubing
- Total time for infusion in minutes
FORMULA: Total vol. x Drop Factor ÷ Total Time (minutes). Answers are in gtts/min.
Administer 1000mL of D5W every 8 hours. Drop factor is 15 (gtts/ mL.)
Administer 500 mL of 0.9% NS over 6 hours. Drop factor is 20
Administer 1000 mL RL over 10 hours. Drop factor is 15
Administer Ancef 1 gm in 50 mL of D5W over 30 min. Drop Factor is 10
Administer IV of 250 mL D5 0.45% NS over 10 hours. Drop factor is 60
1. How many mL/h? 2. How many gtts/min?
INFUSION TIME Total Volume ÷ mL/h.
Pt. to receive 500 mL 0.45% NS to infuse at 25mL/h. Calculate total infusion time.
” ” ” 1000 mL RL at 30 gtts/min, using a drop factor of 15 gtts/min.
- Convert gtts/min to mL/min
- Convert mL/min to mL/h
- FORMULA: Total Volume ÷ mL/h
SUPER COMPLICATED – SEE IF YOU CAN DO IT!
Give dopamine HCL 600 mg in 500 mL D5W at 20 mL/h. Calculate dosage in mcg/min.
Administer Nipride 3 mcg/kg/min. Pt weighs 165 lbs. (Total mcg to be administered per min?)
Total of 50 mg of Nipride ordered, to be diluted in 250 mL of D5W (What is the concentration in mcg/mL?)
Using an infusion pump you would set the flow rate at? (mL/h)
SENSORY SYSTEM EXAM STUDY GUIDE
EYES
DEFINITIONS
Vitreous Humor – Clear, gelatinous material located within the Posterior Chamber. Holds the Retina in place and is part of the Refractive Media of vision. (RM- Cornea, Aqueous Humor, Lens, Vitreous Humor)
Lacrimal Fluid – Tears. Provide oxygen and some nutrients to the Cornea.
Aqueous Humor – Clear, watery fluid located in the Anterior Chamber. Moisturizes and nourishes the Lens and Cornea. Part of the Refractive Media of vision.
Retinal Rods – Photoreceptor cells in the retina of the eye that can function in less intense light than cone cells. More sensitive than cone cells, Rods are concentrated at the outer edges of the retina and are used in scotopic (night) vision, our most sensitive motion detection, and in peripheral vision. On average, there are approximately 125 million rod cells in the human retina.
Retinal Cones – responsible for color vision as well as eye color sensitivity; they function best in relatively bright light, as opposed to rod cells that work better in dim light. Cone cells are densely packed in the fovea centralis, a 0.3mm-diameter rod-free area with very thin, densely packed cones which quickly reduce in number towards the periphery of the retina. There are about six to seven million cones in a human eye and are most concentrated towards the macula.
Ciliary Muscles – a ring of striated smooth muscle in the eye‘s middle layer (Choroid) that controls accommodation of the lens for viewing objects at varying distances and regulates the flow of aqueous humour into Schlemm’s canal. It changes the shape of the lens within the eye, not the size of the pupil. Contraction and relaxation of the longitudinal fibers, which insert into the trabecular meshwork in the anterior chamber of the eye, cause an increase and decrease in the meshwork pore size, facilitating and impeding aqueous humour flow into the canal of Schlemm.
Detached Retina – Injury or trauma to the eye or head may cause a small tear in the retina. The tear allows vitreous fluid to seep between the sensory and pigmented layers, and peel the retina away from the back of the Posterior Chamber like a bubble in wallpaper. A medical emergency, permanent damage will occur if not repaired within 24 – 72 hours. http://upload.wikimedia.org/wikipedia/commons/b/b0/Slit_lamp_photograph_showing_retinal_detachment_in_Von_Hippel-Lindau_disease_EDA08.JPG
Conjunctivitis – Inflammation and/or infection of the conjunctiva. Pinkeye (bacterial). Viral (Herpes Simplex I, Herpes Zoster, Adenoviruses).
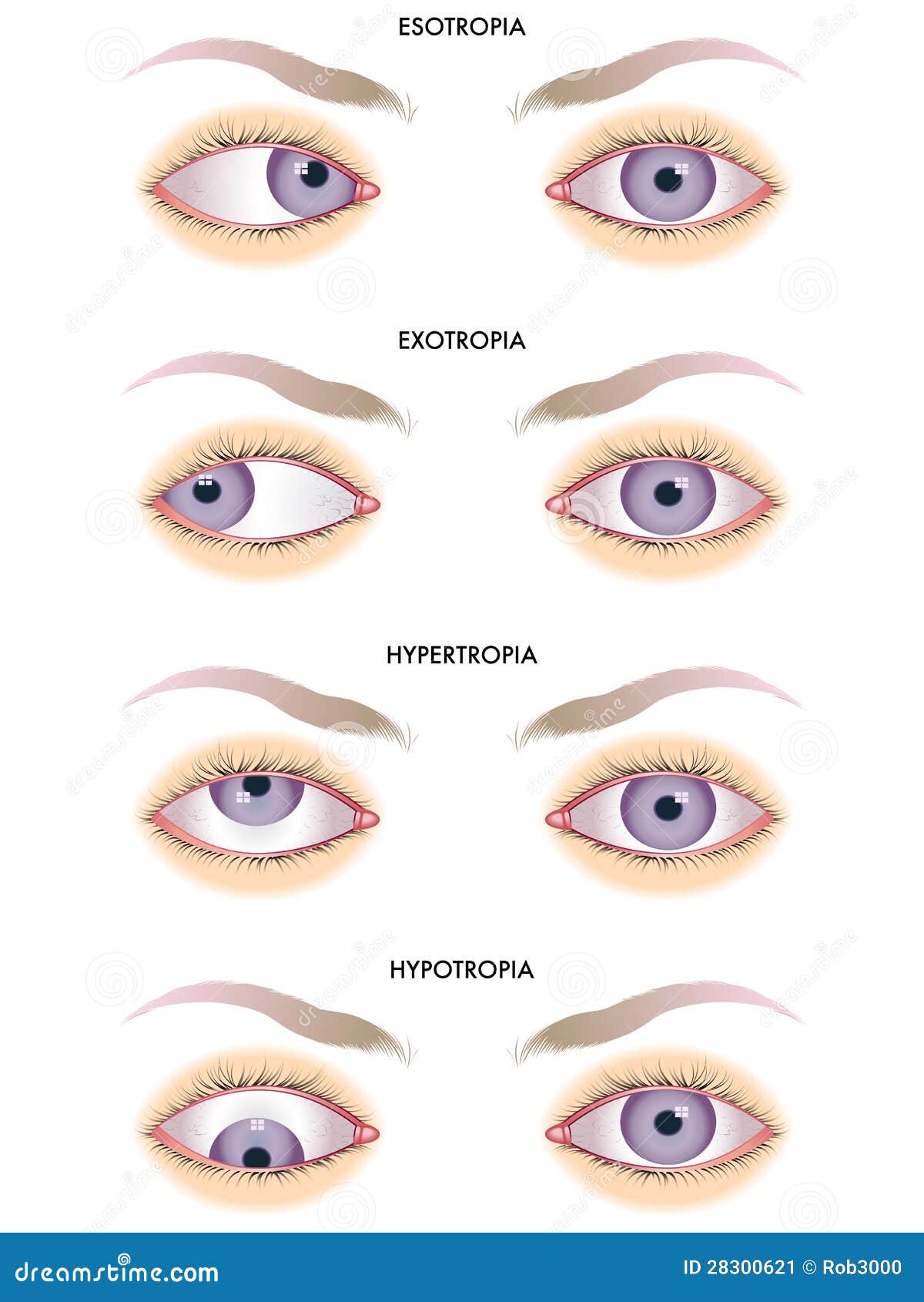
Strabismus – “Lazy eye”. Condition in which the eyes are not properly aligned with each other. Prevents bringing the gaze of each eye to the same point in space, thus hampers proper binocular vision, and which may adversely affect depth perception. http://thumbs.dreamstime.com/z/strabismus-28300621.jpg
Cataract – Clouding of the lens within the eye. Opacification of the lens obstructs light from passing and being focused on the retina. Most common cause of blindness and is conventionally treated with surgery.
Astigmatism – Uneven surfaces of the Cornea or Lens causing distorted vision. May accompany Myopia or Hyperopia. An Error of Refraction.
Stye – Hordeolum. Staphylococcal infection of the eyelid margin originating in a lash follicle.
Myopia – Nearsightedness. Light rays focus in front of retina causing difficulty in seeing distant images. An Error of Refraction.
Glaucoma – IOP increased above normal. Related to interference of outflow of Aqueous Humor via the trabecular meshwork. 2 types – Acute Closed Angle. Chronic Open Angle. http://en.wikipedia.org/wiki/Glaucoma.
Presbyopia – Hyperopia in older people. Poor accommodation of the lens 2º loss of elasticity of the ciliary muscles. An Error of Refraction.
Light enters eye through PUPIL
How does lens bring things into focus? BENDING LIGHT RAYS (REFRACTION) IN ORDER TO FOCUS AND IMAGE ON THE RETINA. Ciliary muscle contracts and relaxes to change the shape of the lens (ACCOMMODATION), permitting the eye to focus on images of varying distances. Contraction – near. Relaxation – far.
What shapes eye? What kind of a ridiculous question is this? Uh, the Vitreous Humor, I guess.
What are the canals of Schlemm for, and what do they do? They are endothelium lined tubes responsible for collecting Aqueous Humor from the Anterior Chamber and returning it to the bloodstream. And that is what they do.
Why is eye exam significant? Another ridiculous question…
Why is it important to know if your client has contacts? And another…
What do you know about color blindness? Only what you taught me, which is NOTHING! Here’s what the National Insitutes of Health have to say about it. http://www.nlm.nih.gov/medlineplus/ency/article/001002.htm
S/S of cataract –
– Clouded, blurred or dimmed vision. Double vision (diplopia) in one eye
– Distortion when looking at distant objects (nearsightedness)
– Painless but intolerant to light (photophobia) and glare
– Difficulty with night vision, ℅ “halos” around lights
– Frequent changes in lens prescriptions
– Colors fading or yellowing of colors
– Lens becomes cloudy, milky white, progressing to yellow and brown
How do you care for a blind person?
* Introduce self to patient, and acknowledge visual impairment. This reduces patient’s anxiety.
* Orient patient to environment. Orientation reduces fear related to unfamiliar environment.
Do not make unnecessary changes in environment. This ensures safety and maintains what the patient has arranged.
* Provide adequate lighting. The use of natural or halogen lighting is preferred to improve vision for patients with diminished vision.
* Place meal tray, tissues, water, and call light within patient’s range of vision or reach. These ensure safety and sense of independence.
* Communicate type and degree of impairment to all involved in patient’s care. This enhances continuity of care.
* Recommend use of visual aids when appropriate. Visual aids such as magnifying glass, large-type printed books, and magazines encourage reading.
* Place food on tray and plate in same place each meal and explain arrangement of food on tray and plate, using clockwise sequence.
* Encourage use of sense of touch. Touch encourages patient to become familiar with unfamiliar objects.
* Explain sounds or other unusual stimuli in environment. Explanations reduce fear.
* Encourage use of radios, tapes, and talking books. Diversional activities should be encouraged. Radio and television increase awareness of day and time.
* Remove environmental barriers to ensure safety. If furniture or wastebaskets are moved, notify patient of changes.
* Discourage doors from being left partially open. Fully open or closed doors reduce the risk for injury among the vision-impaired.
* Maintain bed in low position with side rails up, if appropriate. Side rails help remind patient not to get up without help when needed.
Keep bed in locked position. This prevent falls.
* Guide patient when ambulating, if appropriate. Describe where you are walking; identify obstacles.
* Instruct patient to hold both arms of chair before sitting and to feel for the seat on chairs or sofas without arms. These reduce the risk of falls.
* Consult occupational therapy staff for assistive devices and training in their use.
* Supervise patient when smoking. Supervision prevents accidental fires.
How do you do eye irrigation? Procedure for Eye Irrigation | Nursing Skills / Procedures | Nursing-Nurse.Com.
How do you apply eye ointment?
- Medication Administration Record (MAR)
- Tissue or cotton ball
- Eye Medication (ointment)
- Nonsterile gloves
Nursing Procedures:
Assess the patient and the chart for any allergies
Check the written orders on MAR
Obtains the necessary equipments
Follow the five rights of drug administration
Determine the identification armband
Explain the procedure to the patient
Wash hand and don non-sterile gloves
Gently wash the eye if there is crust or drainage along the margins of inner canthus. (always wipe from the inner canthus to the outer and use warm soaks to soften material if necessary)
- Position patient in a supine position with the head slightly hyperextented
- For Lower Lid:
- With non-dominant hand, separate eyelids with thumb and finger, and grasp lower lid near margin immediately below the lashes, exert pressure downward over the bony prominence of the cheek
- Instruct the patient to look up
- Apply eye ointment along inside edge of the entire lower eyelid, from inner to outer canthus
- For Upper Lid:
- Instruct patient to look down
- With non-dominant hand, gently grasp patient’s lashes near center of upper lid with thum and index finger, and draw lid up and away from eyeball
- Apply ointment along upper lid starting at inner chantus
How do you treat someone with an object stick in the eye? Do not remove impaled object. Stabilize with styrofoam cup, roller gauze. Cover unaffected eye to prevent further injury via conjugate movement.
Postop instructions for cataract surgery? http://bravermaneyecenter.com/dr/POST-OP%20CATARACT%20SURGERY%20CARE.pdf
What postpones cataract surgery? A total of 234 cases (12%) were canceled due to different reasons on the day of surgery. Main reasons for cancellation were poor control of systemic hypertension (77), canceled by patient (46), improper control of diabetes (20), patients did not bring the intraocular lens (18), chest infection or influenza in children (17), local eye infection (13), cardiac problems (11), high intraocular pressure after local anesthesia (8), and uncooperative patients (7). God only knows what’s going to be on the test.
S/S of retinal detachment?
- Painless change in vision (floaters caused by blood cells in the vitreous and flashes of light as the vitreous humor pulls on the retina).
- Photopsia (recurrent flashes of light).
- Blurred vision worsening as detachment increases.
- with progression of detachment, painless vision loss that may be described as veil, curtain or cobweb that eliminates part of the visual field.
- http://www.nursingtimes.net/Journals/2013/02/15/i/w/f/040914Implications-of-and-treatment-options-for-retinal-detachment.pdf
Diamox is used for GLAUCOMA inhibitor of the enzyme carbonic anhydrase. Decreases the secretion of aqueous humor and results in a drop in intraocular pressure.
Contraindicated in situations in which Na+ and/or K+ blood serum levels are depressed, in cases of marked kidney and liver disease or dysfunction, in suprarenal gland failure, and in hyperchloremic acidosis. It is contraindicated in patients with cirrhosis because of the risk of development of hepatic encephalopathy.
Its action is SEE ABOVE.
How do you treat eyes splashed with chemicals? Procedure for Eye Irrigation | Nursing Skills / Procedures | Nursing-Nurse.Com.
What tests indirectly measures intraocular pressure? Tonometry
EARS
Where does the Eustachian tube start and end? Links nasopharynx to middle ear. http://en.wikipedia.org/wiki/Eustachian_tube.
What does the footplate of the Stapes attach to? The oval window. Transmits sound vibrations from the incus to the oval window.
Where are the nerve receptors for hearing located? Organ of Corti, on the basilar membrane separating cochlear duct and scala tympani all contained within the COCHLEA.
What is the true organ of hearing? Organ of Corti.
What is a myringotomy? Surgical procedure creates a small opening in the tympanic membrane to reduce pressure & allow fluid drainage
What is postop tx for myringotomy?
S/S of acute OM are?
How do you take care of a hard of hearing person?
Define conductive deafness and functional hearing loss.
S/S of Ménière’s disease are?
What causes otosclerosis?
Post op care for middle ear surgery?
Where is the malleus?
What is an audiogram?
Where is otitis media found and what is it?
What causes Ménière’s disease?
Where is the origin of motion sickness?
What is a tympanoplasty??
How is hearing loss measured?
How do you pull the ear of an adult for drops?
Nursing Interventions in Eye Disorders and Infections
Nursing Assessment
History (subjective data):
– Change in vision
– Pain, itching, burning
– Excessive watering
– Blurred vision, double vision (diplopia)
– Loss in field of vision, blind spots, floating spots
– Difficulty with vision at night
– Pain in bright light
– Frontal headache
– Halos around lights
– Frequent reddening of eye – conjunctivitis
– Discharge, eye crusted on awakening
– Eyes feel dry- Wearing contact lenses, glasses
– Regular medication
– History of glaucoma in family
– History of diabetes, hypertension
– Date of last eye exam
Physical assessment (objective data):
– Observe for redness of conjunctiva, swelling, secretions, excessive tearing
– Change in visual acuity
– Note any squinting, tilting head
– Note ability to move eyebrows, eyes
Nursing Diagnosis
• Anxiety/fear related to loss of vision
• High risk for infection related to interruption of body surface
• High risk for injury related to visual limitations and unfamiliar environment
• Self care deficit related to post operative
• Knowledge deficit related to post-operative management, medications, and follow up care
Interventions
General interventions for visually impaired
– Speak as you enter the room and before touching patient
– Tell the patient when you are leaving
– Keep door open or closed NOT ajar
– Do not move objects without asking patient
– Give special orientation to room on admission
– Set up meal tray and orient patient to food
Pre-Op:
– Describe procedure – Local anesthetic
– Discharge teaching – eye drops, activity restrictions
– Start stool softeners to prevent constipation/straining
– Wash face well with surgical soap
– Instill eye drops as order
Post-Op:
– Be gentle- no jarring movement
– Treat nausea immediately with antiemetics
– Monitor for pain or visual changes ( sign of bleeding)
– Eye patch with non-allergic tape
– Patch both eye if restricting movement of eye
– Metal eye shield at night for extra protection
– Physician orders for positioning
Instilling Eye Drops
– Verify order (OS, OD, OU)
– Wash hands, give patient tissue
– Remove eye patch, gently cleanse with wet gauze
– Patient supine or head lilted up, look up
– Pull lower lid down
– Squeeze gtts into conjunctiva sac
– Do not touch dropper to patient’s eye
– Put pressure with finger over lacrimal duct to decrease systemic absorption
– Ask pt to close eye gently and rotate eyeball to distribute medication. Do not squeeze eye shunt
– Apply new patch with non-allergic tape
Diagnostic tests for the eye
Ophthalmoscopy: examination of the fundus or interior of the eye done with the ophthalmoscope. (lens, retina, retinal blood vessels, optic disc)
Retinoscopy: determine focusing power of each eye
Tonometry: measures the intraocular pressure (IOP)
Normal IOP = 10-20 mmHG
Visual field examination: measures peripheral vision
Slit lamp examination: binocular microscope magnifies the surface of the eye – iritis, cataract.
Ultrasonography: determine pathologic changes – opaque lens, cloudy cornea, blood vitreous
Retinal imaging: produced high resolution image of the entire retina – diabetic retinopathy
Retinal angiography: detects vascular changes and blood flow through retinal vessels. Water soluble dye used. Special camera used to detect appearance and distribution of dye in the retinal arteries, capillaries and veins.
Infections of the eye
Conjunctivitis: inflammation of the conjunctiva “pink eye” highly contagious. Antibiotic or antiviral ointment or drops, warm soaks or sterile saline irrigation to remove purulent drainage, decrease swelling, relieve pain or itching.
Uveitis: inflammation of the uveal tract – iris, ciliary body and choroid. Oral or topical corticosteroids, mydriatic (dilating) eye drops – atropine, antibiotics, analgesics, sunglasses, to reduce photophobia.
Keratitis: inflammation of the cornea.
Cornea ulcer: erosion in corneal tissue. Topical anesthetics, mydriatrics, local and systemic antibiotics.
Blepharitis: inflammation of the lid margins
Hordeolum or sty: inflammation or infection of the Zeis or Moll gland. Warm soak, topical antibiotic
Chalazion: a cyst of one or more in meibomian glands (sebaceous glands of inner surface of eyelids at the junction of conjunctiva and lid margins). Apply warm soaks, if the cyst is firm – surgically excised.
Cataract Lens becomes cloudy and opaque
Most often as a result of aging (over 50 yrs)
Assessment of Cataract:
– Blurred vision, double vision (diplopia)
– Distortion when looking at distant objects (nearsightedness)
– Painless but intolerant to light (photophobia)
– Difficulty with night vision, c/o glare
– Needs more light for reading
– Colors fading
– Lens becomes cloudy, milky white, progressing to yellow and brown
Treatment and nursing care of Cataract
– Surgery when loss of vision greatly affects quality of life.
– Remove lens and implant new one – local anesthetic
– Monitor for hemorrhage, increased intraocular pressure (IOP), infection
– Increased eye pain, decreasing vision, frontal HA, purulent
drainage, fever and chills
– Do not lie on affected side
– Stool softeners
– Avoid rapid movements, bending from waist
– Assistance with ambulation
Glaucoma
– Increased intraocular pressure (IOP)
– many causes (genetic, trauma, other diseases)
– Damage to optic disc causing atrophy and loss of peripheral vision
– Onset slow or rapid
– IOP determined by aqueous humor
– Excessive production (wide angle glaucoma)
– Decreased outflow (narrow angle)
– Increased IOP restricts blood flow to optic nerve and retina causing ischemia
– If IOP is greater than 23mmHg – evaluate
Closed angle Glaucoma (Acute)
– Sever pain, colored halos around lights, blurred vision, nausea and vomiting
– Causes – iris lies too close to drainage canal blocking drainage of aqueous humor
– IOP rises suddenly (50-70 mmHg)
– Emergency treatment to prevent damage to optic nerve blindness
– Pilocarpine, topical epinephrine
– surgery
Open Angle Glaucoma (chronic)
– More common (over 90% of glaucoma)
– Often inherited, degenerative changes in aqueous humor outflow, usually bilateral
– Symptoms mild until vision is seriously impaired:
– Glasses no longer working
– Blurry vision that clears up
– Trouble adjusting to dark rooms
– Rainbow colored rings around lights
– Narrowing of vision at sides of eyes
Treatment – Drugs of Glaucoma
– Miotics (pilocarpine) constricts pupil, promotes outflow of aqueous humor. Side effects of blurred vision for 2 hrs, difficult adjustment to dark rooms
– Beta-adrenergic blocking agents (Xalatan, Timpotic)
– Carbonic anhydrase inhibitors (acetazolaminde), given orally to decrease aqueous humor production
– Sympathominetics (epinephrine) increases aqueous humor outflow
– Must be taken regularly without interruption
– Will prevent further vision loss but cannot restore vision
– Surgery
– Laser used to create openings so excess fluid can escape, done under conscious sedation
– Post-op: mild headache, blurred vision for 24 hrs.
– Nursing care post-op:
– Monitor for increased IOP – increased pain, HA
– Prevent increased venous pressure in head
– Avoid straining, bending over
– Head of bed elevated, even while sleeping
– No sudden movements

{kind=link}